
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
At every level, Americans spend a lot for health care. It is 18% of the gross domestic product. It is 27% of the federal budget. Employers spend $9,325 per employee on health care annually. American consumers spend an average of $1,514 in out-of-pocket costs per year.
The question is, what do we get for that spend? A recent study commissioned by Kaiser Permanente—Using Mortality & Years-Of-Life-Lost Metrics To Evaluate Health System Performance & Inform Health Care Policy—made me think of that big policy question—and the current state of value-based care.
This is one of just a few studies to measure the “big picture” impact of health services on American consumers. To do this, they compared the mortality rates and years-of-life-lost (YLL) rates of Kaiser members with non-members in those same communities and with the general population of the United States.
Kaiser Permanente members were 35% less likely to die early than the comparison groups when looking at all causes of death combined. And mortality rates among Kaiser Permanente members were lower than nonmembers in the community for all racial and ethnic groups.
There can be many hours of discussions about these types of studies, their design, and the findings. But a related issue is the question: As we move away from fee-for-service to value-based care (VBC), what should we measure? How do we quantify and pay for “value”?
The lack of answers to these questions are a consistent concern of executives in the field. The issue is that the default for “value” is focused on spending—emergency room use, admission rates, readmission rates—and not clinical outcomes (see VBR Sputter or Surge?).
Stakeholders want to “measure something that matters”—but there are few widely-adopted standardized measures of clinical outcomes. For high-needs consumers with behavioral health conditions, there is growing interest in using measurement-based care (MBC) approaches to both measure and manage clinical outcomes. This was the focus of the presentation of my colleague, OPEN MINDS Senior Advisor Stuart Buttlaire, Ph.D., during Measuring What Matters—An Update On Patient-Centered Outcomes and Feedback Informed Care, which took place at The 2025 OPEN MINDS Service Excellence Institute.
In the opening of the session, Dr. Buttlaire framed the issue, “Measurement-based care and feedback-informed care are core elements of evidence-based practice and shifting organizational clinical culture. We need to extend that thinking into contracting with payers. If provider organizations are going to compete for consumers and contracts—and participate meaningfully in value-based reimbursement—they must be able to demonstrate impact beyond utilization metrics.”
Dr. Buttlaire provided a context for thinking about MBC and measuring value. “Measurement-based care is not simply a collection of outcome tools. It is a clinical process. It refers to the systematic use of standardized, validated tools that are consistently and repeatedly administered, reviewed in real time, and used to guide treatment decisions. The key is to embed the process in clinical workflows.” He emphasized that MBC is broader than any specific scale or tool—it is a process. It is not just data collection. Rather, it is about integrating measurement into clinical decision making.
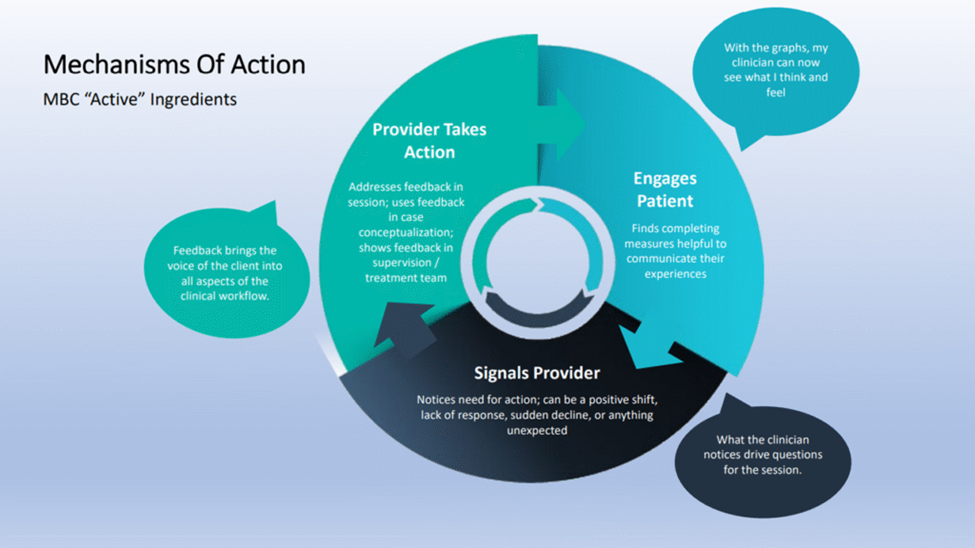
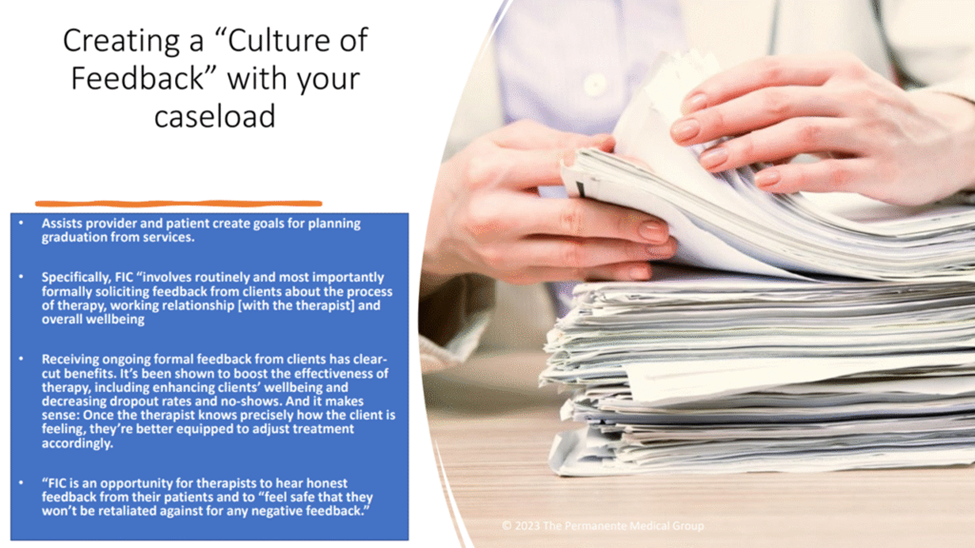
Within the context of MBC systems, Dr. Buttlaire is an advocate of feedback-informed care (FIC) models. He said, “Feedback-informed care is focused on consumer-reported outcomes that are used to build a therapeutic alliance and provide a structured approach for feedback between consumer and clinician. Most simply, all feedback-informed care models are a form of measurement-based care—but not all measurement-based care uses feedback-informed models. What distinguishes feedback-informed care is the intentional use of therapeutic alliance and outcome feedback during sessions to adjust care in real time.”
His observation is that there are plenty of tools to measure outcomes and clinical status—they just lack consistent implementation. Dr. Buttlaire noted that for adult populations, symptom tools such as PHQ-9 or GAD-7 are commonly used. And for child and adolescent populations, two measures are especially relevant: the CANS (Child and Adolescent Needs and Strengths) and the PSC-35 (Pediatric Symptom Checklist). Within FIC, tools such as the Outcome Rating Scale (ORS) and Session Rating Scale (SRS) are common.
To get started with MBC and measuring value, Dr. Buttlaire recommended a few key steps. First, start small, selecting two or three measures aligned with core populations. Then, integrate the MBC process into workflows (intake, periodic reassessment, supervision review) and display the data in simple dashboards. Finally, use the data in supervision and case review.
He closed the session with an observation for clinical leaders: “If quality measurement is only done for payer reporting, clinicians resist it. If it is used to improve care and engagement, it gains legitimacy.”