
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
Greetings from Clearwater Beach and the 2026 OPEN MINDS Performance Management Institute. This week, while I’m here with 650+ executives focused on performance optimization of programs serving high-needs consumers, Aledade announced it had added 700 primary care provider organizations to its networks for its 2026 value-based contracts. This brings their network to 3,000 primary care provider organizations serving 3 million consumers.
The growth of Aledade is attributed to both a changing payer landscape and provider organization strategy. On the payer side, part of this growth is driven by an increasing number of Medicare beneficiaries in accountable care organizations (ACOs)—14.3 million people are enrolled in an ACO as of January 2026, up by 4.4% from 13.7 million in 2025. That brings total participation in these Medicare Shared Savings Programs to 511, up from 476 ACOs in 2025.
In addition, in 2025, CMS introduced several new payment models. While the ACO REACH model will conclude this year, CMS announced the LEAD, or Long-Term Enhanced ACO Design, model as its successor. The 10-year voluntary demonstration officially begins January 1, 2027 and will run through December 31, 2036. All of this Medicare movement comes at a time of increasing investor interest in value-based care with a string of new investments.
For provider organizations serving high-needs consumers—those with behavioral disorders, cognitive disabilities, and health-related social needs—this movement toward more Medicare value-based reimbursement (VBR) is an opportunity. There will be more acceptance of capitated primary care-centric VBR models in Medicare, which often drives new model development in Medicaid and commercial health plans. And most of the current ACO models are not designed to serve these consumers. But VBR contracting with specialty provider organizations is glacial—constantly moving but slow.
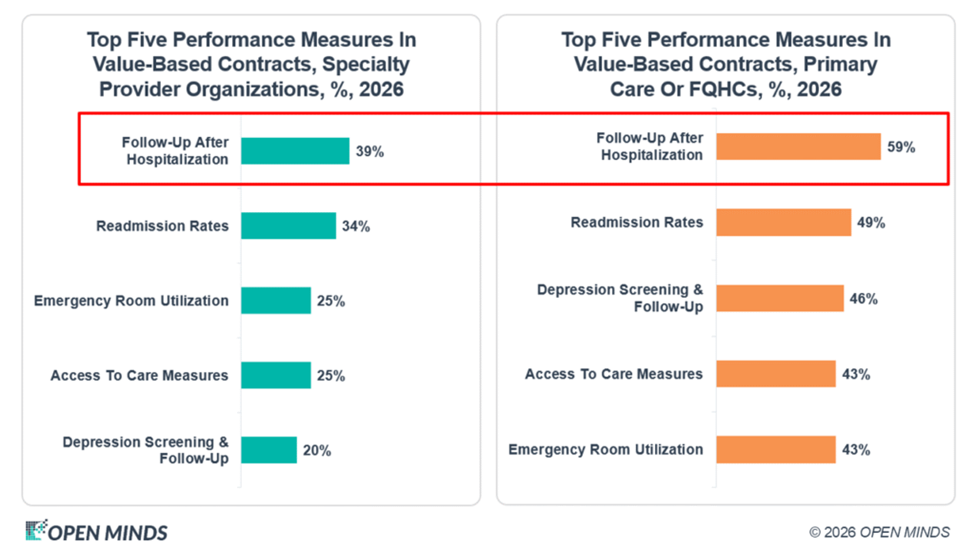
Our recent survey of performance management in the field—The 2026 OPEN MINDS Performance Management Executive Survey: Where Are We On The Road To Value—provides a snapshot of the evolution in performance-based contracting in this sector of the field. Most importantly, 81% of primary care organizations have VBR arrangements with health plans, compared to 65% of specialty care organizations. In these arrangements, follow-up after hospitalization and readmission rates were the most common performance measures, with data management and IT infrastructure remaining the greatest impediments to success with VBR.
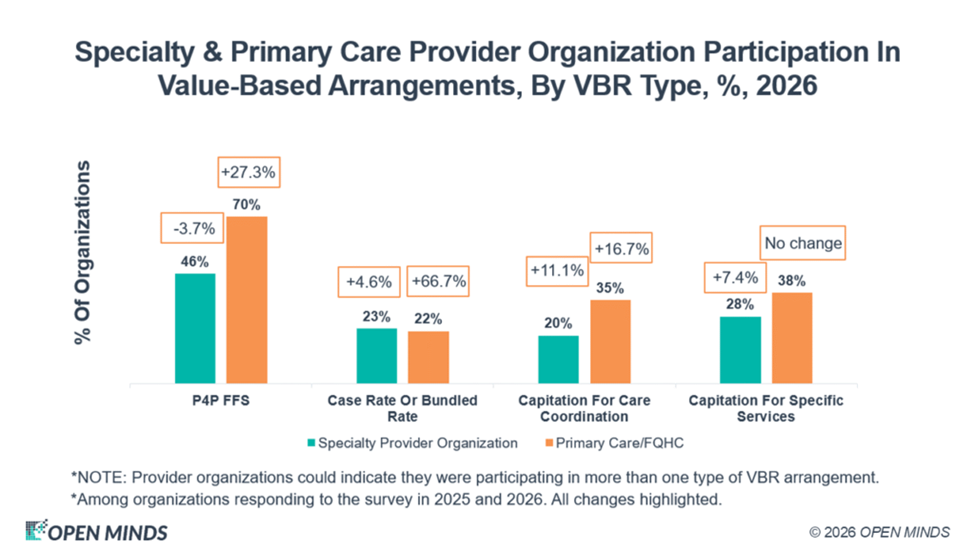
Within these numbers are some important variants. About 25% of specialty and primary care organizations have some type of case rate contract, while 28% of specialty care organizations and 38% of primary care organizations, respectively, have capitated contracts of some sort. And 63% and 32% of specialty organizations and primary care organizations, respectively, have 20% or more of their revenue from VBR arrangements.
The issue for executive teams serving the high-needs population is that value-based care with meaningful gainsharing will likely require whole person care models that include primary care and downside financial risk of some type. To make this opportunity a reality, leadership teams will need to restructure their relationships with payers and health plans, strengthen their value-based management infrastructure capabilities, and develop a team (and an organization) with a population health mindset.
In an interview, Farzad Mostashari, M.D., co-founder and CEO of Aledade, observed, “This administration has made it clear… that they want more and more patients in traditional Medicare to be cared for better in value-based arrangements like ACOs.” The CMS desire to move away from fee-for-service is echoed by provider organization executives. Mat Kendall, co-founder and president at Aledade, noted, “There’s really strong desire by providers of all sizes in all parts of the country to get rewarded for providing high-quality care, and these models are now working…the common element all of this is really this desire to help their patients and to get rewarded for it.”
With the likely financial pressures in the field in the year ahead, the demand for new models to serve high-needs consumers will increase—and the question is: What organizations will fill that market white space?