
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
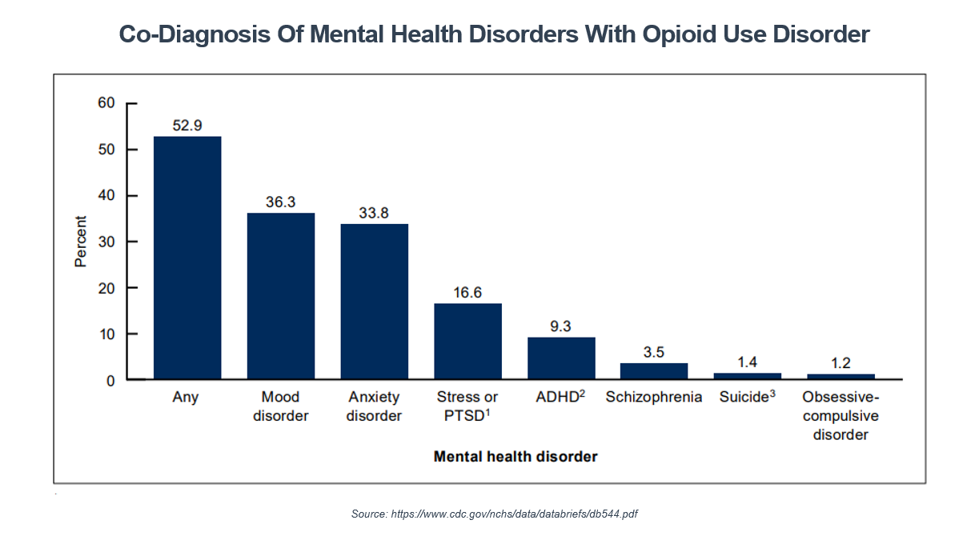
Greetings from “The Big Easy” and the first day of the 2026 OPEN MINDS Strategy & Innovation Institute. I spent the day with 500+ executives focused on innovation as the strategic path to sustainability in this changing market. The day opened with a great keynote session with Debra Nussbaum, Ph.D., Senior Director of Behavioral Health Evidence Based Services, National SUD Strategy Lead with Optum, Inside The Payer View: The Future Of Addiction Treatment Service Delivery. Her perspectives underscored the complexities of addiction treatment in the current market. This is due in part to the fact that for adults with an opioid use disorder (OUD), over half (52%) have a co-occurring mental health condition. Over a third have a mood disorder (36%) and/or an anxiety disorder (34%) – the findings of a newly published analysis – Health Center Visits By Adults With Opioid Use Disorder: United States, 2023.
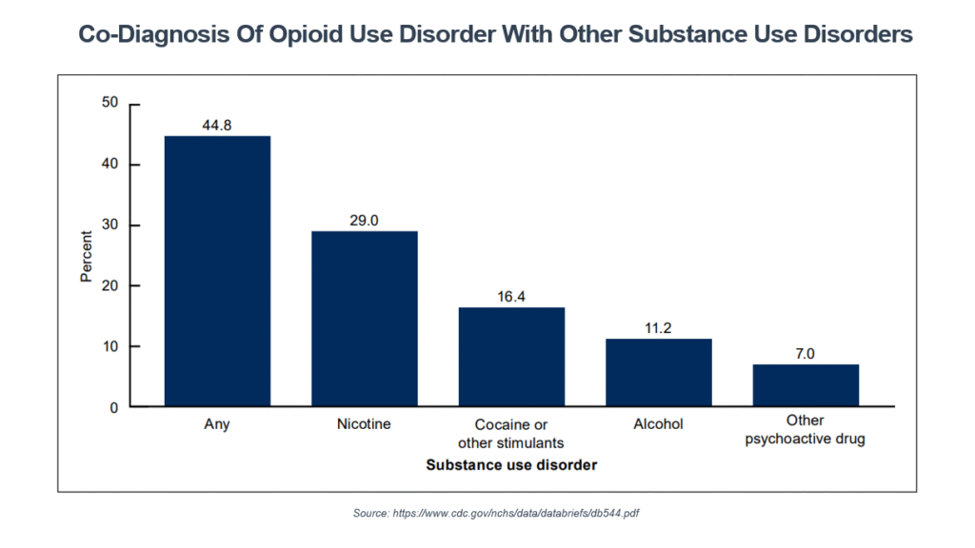
The research also found that among adults with OUD, 16.6% had a co-diagnosis of severe stress or post-traumatic stress disorder; 9.3% had attention-deficit/hyperactivity disorder; and 3.5% had a schizophrenia diagnosis. The same research also found significant prevalence – at 44.8% – of co-occurring use of other substances. This includes a 29.0% use of nicotine, cocaine or other stimulants at 16.4%, and alcohol at 11.2%.
This data illustrates the challenges of helping consumers recover from an OUD – and the need for innovative treatment approaches. That was the focus of a recent RECADEMY webinar, Integrating Psychiatric & Substance Use Disorder (SUD) Treatment: Models, Evidence & System Transformation Opportunities. Louai Bilal, M.D., Medical Director of the Kaiser Fremont Medical Psychiatric Unit; Charles Whitehill, M.D., Chief of Addiction Medicine and Recovery Services (AMRS) for Kaiser Permanente Napa/Solano; and my colleague Stuart Buttlaire, Ph.D., OPEN MINDS Vice President of Clinical Excellence and Leadership, discussed how to create better treatment experiences and outcomes for these consumers.
These clinical experts focused on the need to “replace” some elements in traditional addiction treatment models for better outcomes for consumers with OUD. What should be replaced? In their opinion, sequential treatment, siloed specialists, and narrow entry points need to go for success with OUD treatment.
First, replace sequential treatment with simultaneous treatment. Dr. Whitehill defined sequential treatment as a model that postpones mental health treatment until a consumer’s substance use disorder has stabilized. He explained that sequential care can miss diagnoses and prolong instability, causing consumers to continue using substances to “self-medicate,” leading to a potentially worsened psychiatric condition. Instead, clinical leaders should design models to start psychiatric assessment, stabilization, and treatment while they assess substance use and start detoxification or relapse prevention medications. Rather than sending consumers to a series of disconnected referrals for “the next level of care,” these integrated approaches can reduce service gaps when relapse, readmission, and mortality risks are highest. “It’s very common to see sequential care,” said Dr. Whitehill. “We postpone mental health treatment until this person is stable. That creates a problem because you’re going to probably miss a significant diagnosis of something that’s going on. You’re going to have somebody who’s much more difficult to stabilize. Either the substance use disorder doesn’t get stabilized or the mental health disorder gets destabilized by ongoing use. So right at the start, when you do sequential care, you’re leaving out half of the problem and expanding the time, energy, and resources needed to take care of that.”
Second, replace siloed specialists with a multidisciplinary team that can share responsibility for the consumer over time. This means building a team with clinical professionals who have different skills and can conduct regular case conferences and shared treatment planning through a shared electronic medical record.
“For a chronic care condition like substance use that is comorbid with psychiatric disorders, you really do need a multidisciplinary team because the care requires different skill sets,” said Dr. Bilal. “One infrastructure point to support this, which is now self-evident, is an electronic medical record (EMR) integrated across specialties. And you need [clinical] relationships across different settings, whether it’s a hospital, the clinic, the residential program, or the community, and a mode to communicate with all those teams.”
Finally, replace narrow entry points with a “no wrong door” system. Executives need an approach that provides access to treatment wherever the consumer enters the system – such as an emergency department, an intensive care unit, an inpatient psychiatric unit, a hospital floor, an outpatient clinic, or a community-based program. Critical elements to help this approach are “navigators” who can help move consumers through the system to the right level of treatment and reduce referral barriers.
“Looking at your individual systems and going with that mentality of no wrong door to access and see where you can improve access to care within your system in each respective clinic, emergency room, hospital floor, or community-based [location],” said Dr. Bilal. “Wherever your patients are, try and give them an access point to treatment.” For executives serving consumers with an OUD, this restructuring of the treatment model is a necessity to improve outcomes and reduce total costs of care. The restructuring will require a deliberate plan and an investment – but will reflect the emerging best practices in the field. As Dr. Whitehill put it, “Start with a very clear plan of what you want to do, make a commitment to integration, and start small. Start small and have patience for results.”