
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
There has been a lot of confusion about how last year’s Congressional budget bill, coined the One Big Beautiful Bill Act (OBBBA), signed into law on July 4, 2025, will affect Medicaid this year. And for good reason, there are 12 very significant provisions in the bill affecting Medicaid—each with a different impact on Medicaid policy, regulations, and funding.
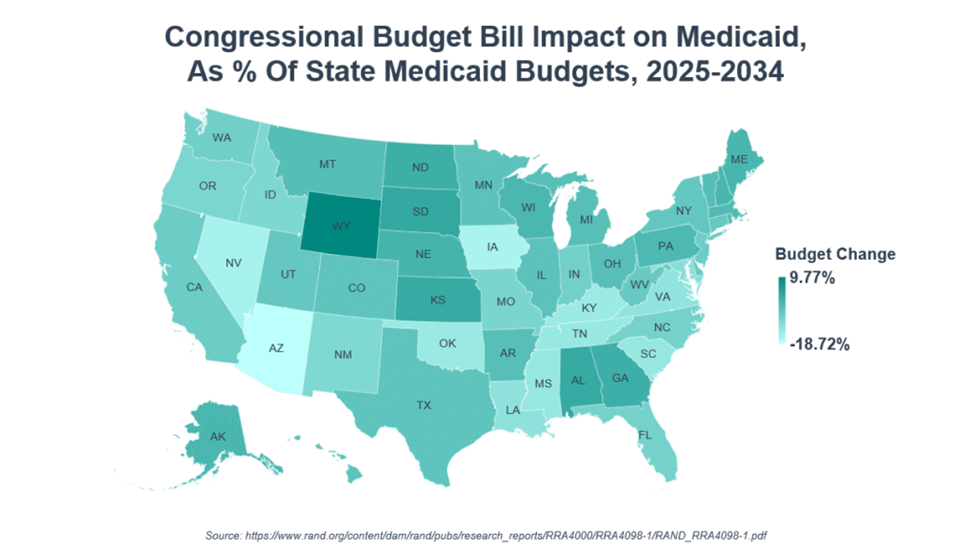
A recent analysis—State-Level Impacts Of Key Medicaid Provisions In The One Big Beautiful Bill Act—projected the likely impact on the field. At the macroeconomic level, state Medicaid budgets are expected to be cut by $664 billion over the 2025–2034 period—this is approximately $1.33 billion per year per state during this time period. (The reduction in federal spending during the same time period is estimated to be $714 billion.)
But the impact will vary greatly by state—with 26 states expected to see reductions of 5% or more. Expansion states with substantial use of state-directed payments (SDPs) and provider taxes—Arizona, Iowa, and Nevada—are expected to see reductions of more than 15% of their Medicaid budgets. California and New York similarly have substantial use of SDPs and provider taxes and will see the largest dollar-value reductions, on the order of $112 billion and $63 billion, respectively.
As a non-expansion state without substantial use of SDPs or provider taxes, Florida will see minimal budgetary effects. Funds expected from the Rural Health Transformation Program (RHTP) will temporarily offset the losses in some states. For example, South Dakota and Wyoming, will see slight increases in Medicaid budgets—2% and 10%, respectively—as their small populations and smaller Medicaid budgets mean they will gain funding from RHTP.
One issue of particular import for provider organization executive teams is the curtailment of state-directed payments. Since 2016, CMS has allowed states to set the rates that Medicaid health plans pay to provider organizations rather than using Medicare rates as a benchmark. The Congressional budget bill repeals this arrangement—and will eliminate SDPs in new waiver applications and renewals—and will reduce the upper payment limit by 10 percentage points each year until parity with Medicare is achieved.
These supplemental provider rates, in 24 states, were worth $3 billion in additional payments in 2025. The rates vary from 36% to 300% more than Medicare rates, with the median being nearly twice the Medicare rate. South Carolina and Nevada had the highest mean SDP rates relative to Medicare in 2025—at 280% and 251%, respectively. Texas and Tennessee will see the largest reductions to SDP amounts in dollar terms, at $19.7 billion and $15.9 billion, respectively, over the years 2025 to 2034. And Tennessee, Mississippi, and South Carolina state Medicaid budgets will be reduced the most by the curtailment of SDPs. In total across all states and years, the reduction of provider payments represents a reduction in Medicaid spending of $241 billion through 2034.
With Medicaid covering 26% of the U.S. population and making up 18% of total U.S. health care spending, the effects of federal policy changes on the Medicaid program have a significant impact on the field. Our team will continue to cover the developments—and what they mean for health and human services executives.