
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
About 3,900 school-based health centers (SBHCs) operate across the United States, providing primary care and behavioral health services directly in schools. Despite their visibility in health policy discussions, these programs represent a relatively small proportion of the approximately 100,000 public schools in the United States. Approximately 6.3 million children receive health services at school each year.
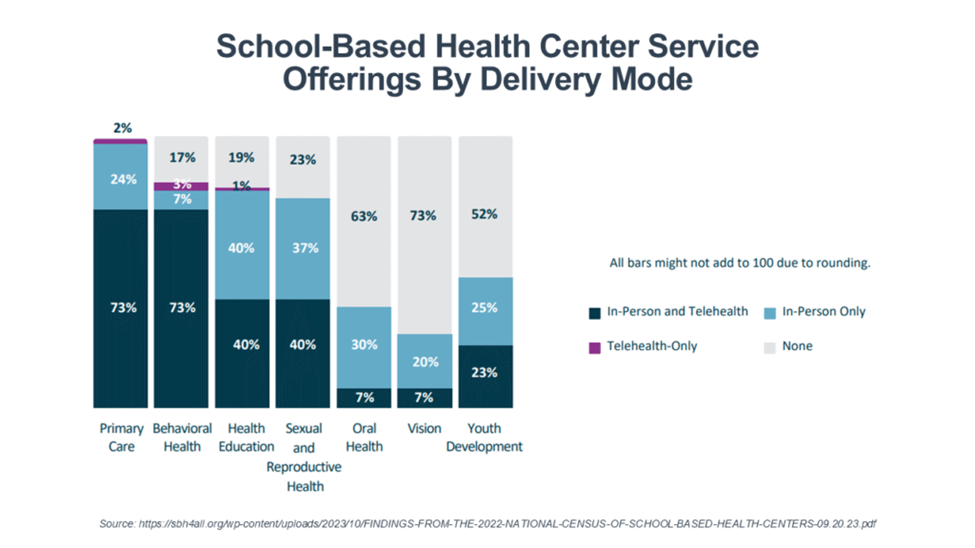
The majority of SBHCs offer primary care and behavioral health services on-site—almost 75%. Most (65%) are sponsored by federally qualified health centers (FQHCs). And for most SBHCs, revenue comes from billing and third-party insurance claims (74%), followed by federal funding (55%), in-kind support (33%), private foundation funding (21%), local government funding (15%), and school-system funding (14%).
But there are concerns that reductions in Affordable Care Act subsidies and Medicaid eligibility requirements may threaten the financial sustainability of SBHCs. The changes in federal policy may also jeopardize the ability of schools to bill Medicaid for therapeutic services such as speech, occupational, and physical therapy, as well as assistive technologies for children who are Medicaid recipients.
The challenge—and the future role of school-based health services—was discussed during the session Back To The Future: How Today’s Health Care Is The Realization Of A 1990s Vision at The 2026 OPEN MINDS Performance Management Institute. Mary Lauren Salvatore, executive director of Education Plus Health, outlined how integrated school-based care models are evolving as health care and education systems confront a changing reimbursement landscape.

Education Plus Health, founded in 1982, is a nonprofit provider organization with approximately $3.5 million in annual revenue that serves more than 7,000 students across 11 schools and school-based health centers in charter, public, and private schools, along with more than 300 families of children with asthma through partnerships with the Philadelphia Department of Public Health and pediatric practices.
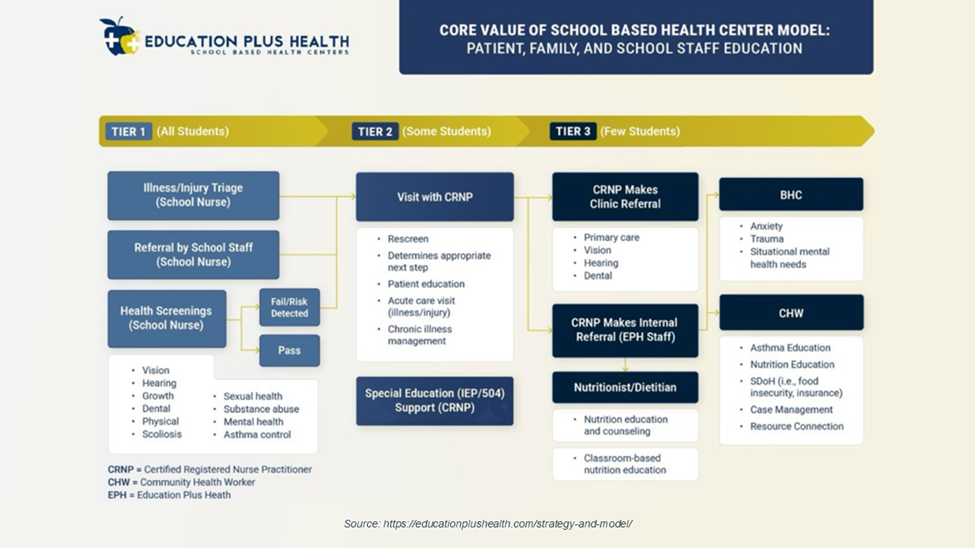
The Education Plus SBHC model is nurse practitioner-led and embedded directly within participating schools–both charter schools and private schools in Philadelphia. Care teams include nurse practitioners, school nurses, behavioral health counselors, and community health workers, creating an interdisciplinary model designed to address both clinical needs and the broader social determinants affecting student health.
In addition to clinical care, the program includes youth-focused prevention initiatives and public health programming delivered within the school setting. This includes nutritional education, insurance navigation, and social determinants of health support. Ms. Salvatore noted that by locating services where students already spend most of their day, the model reduces barriers such as transportation, scheduling challenges, and the stigma often associated with seeking behavioral health services.
“This structure creates a seamless continuum of care, eliminates fragmentation, and fosters trust and familiarity within the school community,” Ms. Salvatore said. She added that this happens by ensuring students receive whole child support in a setting where they already spend most of their time. Over the past decade, policymakers and educators have increasingly linked student health with academic performance. Ms. Salvatore pointed to the Centers for Disease Control and Prevention’s Whole School, Whole Community, Whole Child framework that aligns education, public health, and school health sectors to take a whole-child approach to improve learning and health. This model “prompted states and local education agencies to expand health promotion efforts within schools, recognizing that healthier students are better positioned to achieve academically,” Ms. Salvatore said.
The COVID-19 pandemic accelerated this shift as school leaders saw firsthand the effects of limited access to physical and mental health services on student well-being and learning outcomes. She said that since then, there has been “substantial” growth in funding for school-based mental health programs and the expansion of SBHCs nationwide, reducing barriers to care such as transportation, time, cost, and stigma. “Today, school-based health care is increasingly viewed not as a supplemental support, but as an essential component of educational infrastructure,” Ms. Salvatore said.
When asked how school-based services may evolve over the next few years, Ms. Salvatore observed that with the potential loss of Medicaid coverage for many American families, school-based primary care will play an increasingly critical role in maintaining access to health care for school-aged children. This will increasingly happen through partnerships between primary care provider organizations and school systems.
She summarized this future view: “In the coming years, school-based services will likely evolve into a central strategy for protecting child health, reducing disparities, and ensuring that disruptions in the broader health care system do not compromise student well-being or academic success.”