
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
Addressing health-related social needs reduces the total cost of care. That was the central finding of a recently released evaluation of accountable health communities—Accountable Health Communities (AHC) Model Evaluation.
The accountable health community model was launched in 2017. In the study, 28 organizations were paid to provide Medicaid and Medicare beneficiaries with screening for unmet health-related social needs; referred consumers to community services to address those needs; and provided navigation support to assist those consumers in accessing those services. The model focused on five HRSNs: housing instability, food insecurity, transportation problems, utility difficulties, and interpersonal violence.
There were two accountable health community models. One—the assistance track—provided the basic screening, referral, and navigation services. The other—the alignment track—also added community stakeholder engagement. The assistance track resulted in a 3% reduction in total expenditures for Medicaid beneficiaries and a 4% reduction for Medicare beneficiaries. For the alignment track, the Medicaid beneficiary reduction in total expenditures was 4%.
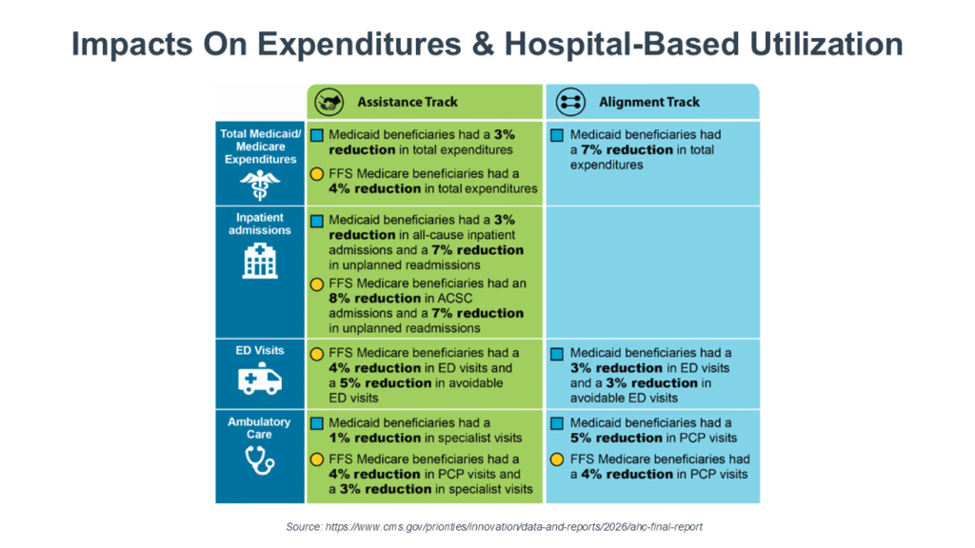
This total cost of care reduction was due to a 3% and 8% reduction in all-cause readmissions for Medicaid and Medicare beneficiaries, respectively. For Medicaid beneficiaries, there was a 3% reduction in emergency department (ED) visits and a 3% reduction in avoidable ED visits. For Medicare beneficiaries, these reductions were 4% and 5%, respectively. A more granular look at the data found a greater impact for dually eligible consumers and for consumers with behavioral health and chronic health conditions.
Not surprisingly, the impact of addressing health-related social needs had a larger effect on the population participating in Medicare alternative payment models. The study authors attribute this to “some beneficiaries […] in APMs receiving enhanced care management services alongside the navigation services provided through the AHC Model […] Navigators performed complementary functions as a care manager or care coordinator for their clients […] in addition to their work connecting beneficiaries to community-based organizations. These care management and care coordination services combined with navigation services may have had synergistic effects on the cost and utilization outcomes.”

These new findings highlight the potential of, and challenges to, meeting health-related social needs (HRSNs) in the changing policy landscape. This was the focus of a recent webinar, How Social Determinants Of Health Are Shaping Health Plan Strategies For Whole Person Care, featuring my colleagues, OPEN MINDS senior associates Margaret Mays, Ph.D., and Sharon Hicks. The takeaway from their discussion is that recent changes in federal policy will not eliminate funding for HRSNs—but will move the contracting and reimbursement for those services to a health plan-specific basis.
Ms. Hicks discussed how, in 2022, the Centers for Medicare and Medicaid Services (CMS) issued guidance adding services addressing HRSN to covered Medicaid benefits through the 1115 waiver program. This has resulted in increased state coverage of housing supports, nutrition support, and transition programs for incarcerated consumers. But in 2025, CMS rescinded prior guidance that had explicitly encouraged states to use Medicaid authorities for HRSN interventions.
As she noted, “This changed the broader framework by creating a “case by case” model for approval rather than the standardized approval that was in place before. However, even with these new parameters, there is still support for HRSN programs as long as they can demonstrate budget neutrality and reductions in medical expense.”
For example, Ms. Hicks noted that while CMS has ceased funding of the “housing first” model, they are still approving HRSN programs that include housing. “In fact, California, New Jersey, North Carolina, and Oregon have each had new 1115 programs that include housing receive CMS approval since 2025,” said Ms. Hicks. “These new programs are explicitly targeted to specific high-risk populations and to medical outcomes.”
Another example of the continued expansion of the programs addressing HRSNs is the development of “Food As Medicine” services. Centene recently called on CMS to “remove unnecessary barriers” preventing Medicare Advantage plans from providing “Food As Medicine” benefits. And a wide range of payers—including Anthem and Elevance—have investments in this area.
For provider organization executives, health plans are going to remain focused on how best to reduce the costs of care for high-needs consumers with chronic conditions—and addressing HRSNs is a proven method to do just that. To evaluate the feasibility of those market opportunities, Ms. Hicks recommends a structured process that includes assessing health plan needs; estimating where social service supports can have maximum impact; and designing service models and estimating the ROI of those services.
Ms. Mays added, “Some health plans are using “in lieu of” services to cover housing and food programs, and using existing stratification models to identify ‘high needs’ populations or those with complex needs to prioritize receiving additional services for housing and food programs. Many plans proactively reach out to providers when one of their patients has been identified as high risk or complex and they usually provide this information on their secure provider portal. In addition, providers should contact their health plan network representatives for more details on these and other new initiatives.” Both speakers emphasized the importance of knowing the metrics of any proposed social support service—its cost, its target consumers, and the likely impact on clinical outcomes and cost. As Ms. Hicks put it, “Executives must demonstrate their outcomes based on the overall medical spending or overall disease acuity models that are currently required by CMS. Data collection, reporting, and cost models will need to become part of every program.”