
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
A little over 5% of all emergency department visits (5,215 of 100,000 visits) in the U.S. were for mental health issues. And these visits vary by both consumer age and diagnosis, according to new data—Mental Health-Related Emergency Department Visits—released by the Centers for Disease Control for March 2026.
Most of the mental health emergency room visits are for anxiety (4% of the total). This is followed by depression (3%), bipolar disorder (1%), schizophrenia spectrum disorders (0.8%), and trauma (0.6%).
The highest rate of mental health-related emergency department visits was among youth aged 12 to 17 (7,464 per 100,000 emergency department visits), followed by adults aged 35 to 64 (6,186 per 100,000), adults aged 18 to 34 (6,004 per 100,000), and consumers 65 and older (4,853 per 100,000).
The age pattern varies by diagnosis. Anxiety-related visits were highest among adults aged 35 to 64 (3.1% of emergency department visits within that age group). Depression-related visits were highest among youth aged 12 to 17 (2.6%), and trauma-related visits were also highest among youth aged 12 to 17 (1.0%). Bipolar disorder and schizophrenia spectrum disorder visits were highest among adults aged 35 to 64 (0.7% and 0.7%, respectively).
Because emergency room costs, in total, are over 2% of total health care spending and 50% of admissions start with an emergency room visit, payers and health plan executives are very focused on how to address consumer health crises and prevent hospitalization. We got a firsthand look at one strategy to do just that—developing a mental health crisis response function outside of the emergency room—in the recent webinar, Breaking The Revolving Door: How An Intensive Crisis Stabilization Center Is Reducing ER Reliance, with Jaclyn McCarthy, vice president of program excellence, and Nancy M. Manigat, chief operating officer at Central Nassau Guidance & Counseling Centers (CN Guidance).
Headquartered in Hicksville, New York, CN Guidance is a $46 million provider organization offering a range of behavioral health and substance use disorder services, including crisis stabilization, care management, outpatient treatment, residential services, and community-based supports. The organization employs approximately 400 staff and serves approximately 30,000 consumers per year.
The CN Guidance executives spoke to how emergency department (ED) visits in the region were increasingly due to individuals presenting with untreated mental illness, substance use disorders, and homelessness. At the same time, outpatient access for behavioral health treatment remained limited with long wait times.
As Ms. Manigat noted, “There was an increase in instances of untreated mental illness on the streets, in the subways, and on the railroads—and also a prevalence of more potent fentanyl on the streets. But while the emergency room is designed for acute, life-threatening care, it’s not designed for mental health crises.”
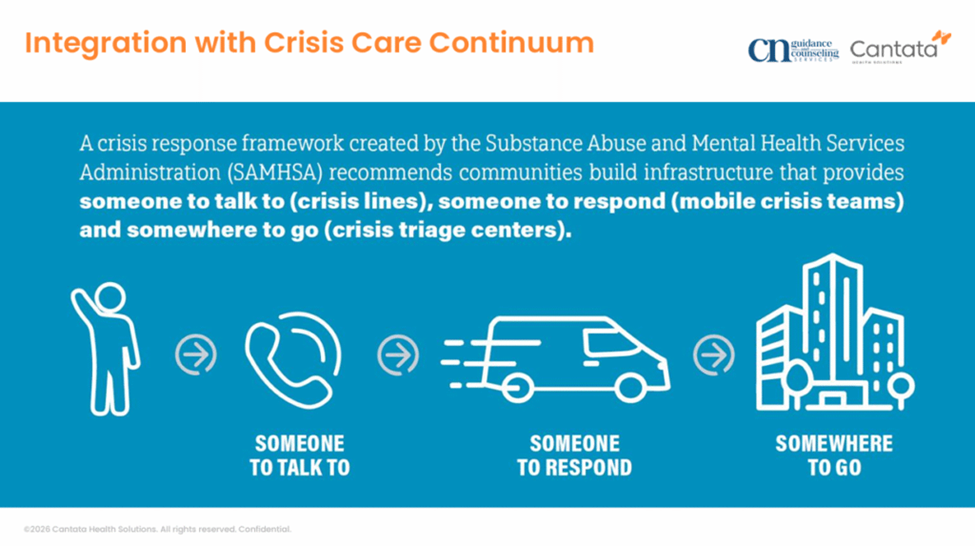
For the CN Guidance team, the situation created the need for a different front door for consumers in a behavioral health crisis—one designed for rapid behavioral health assessment, stabilization, and connection to ongoing care. To meet that need, they developed the Community Crisis Center (CCC), an intensive mental health crisis stabilization program. The model, funded by $1.5 million in annual New York State funding, is designed to function as part of a broader crisis continuum, not as a stand-alone site—with community involvement from hospitals, schools, law enforcement, and social services central to the program’s design.
The CCC program is built around immediate triage, short-term observation, and direct connection to the next level of care. Consumers arriving at the center are assessed by trained staff to determine whether the crisis is related to mental health, substance use, or both. Services provided include medication-assisted treatment, ambulatory detox for mild and moderate substance use, observation and stabilization, treatment referrals, and safety planning. The physical space itself is trauma-informed, with private rooms and shared, home-like spaces designed to reduce distress and support engagement. Even operational details—from separate workflows for law enforcement to showers, snacks, and quiet spaces—are intended to make the setting feel fundamentally different from both an emergency department and a correctional environment.
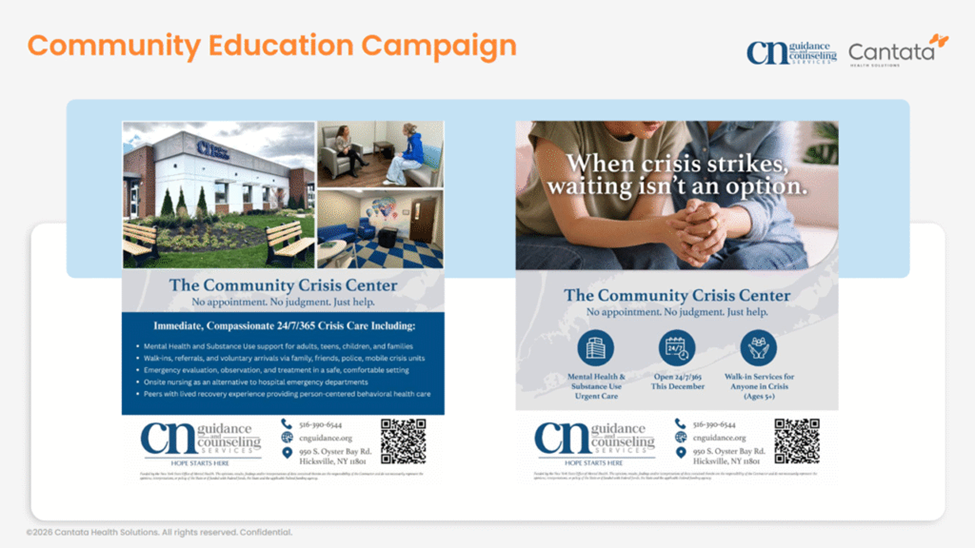
“The CCC is there for on-demand treatment for people who are ready and willing to get help,” Ms. Manigat said. “So, whatever time of night, whatever day, when they are ready, we are there.”
Since opening in December 2025, CN Guidance has served 262 consumers with the new CCC approach, 13% of whom returned for services more than once. Of those served, 12% were diagnosed with substance use disorder, 36% had anxiety or depression, and 12% presented with suicidal ideation or self-harm.
The speakers shared two “essentials” for replicating their approach. First, a crisis center needs to be built as part of the community crisis continuum. And, secondly, in building a budget model for a crisis center, the functionality (and costs) of the technology infrastructure needs to be considered from the outset.
The executives emphasized that for successful outcomes, any crisis center model needs partnerships with the local community. And they underscored the need to work with these partners—such as hospitals and other specialty provider organizations—early in the process to build the needed referral pathways.
“We have been working within our existing crisis continuum from the minute that we knew that this was going to be an RFP and we were interested in going for it,” said Ms. McCarthy. “We engaged all of those providers in the very beginning. As soon as we got the award, from that day until after we opened, we’ve been engaging them in conversations. We set up a stakeholder group that includes all of these folks—our 988 provider, our local hospitals, our mobile crisis team, some school districts, the police department, Homeland Security, and religious organizations.”
The other issue is addressing the technology and reporting functionality needed for crisis management success. They stressed that the crisis center team needs the ability to share consumer data and generate billing documentation. In addition, staff need the data to manage the performance of the crisis center—from referral sources and wait times to consumer dispositions and outcomes.
“Crisis services are fast-paced,” said Ms. McCarthy. “Clients are in and out, so the turnover is very fast. The documentation is done very quickly. You need to be able to have an electronic health record that can generate reporting and give you information just as fast as you’re putting it into the system. And make sure you are looking at where the future of the services is going. You may be building a program today that hits the needs of today, but our needs as communities are constantly changing.”
Both executives emphasized that “emergency room alternatives” run the risk of failure if they are simply another siloed service—and building a well-connected community crisis infrastructure strategy is a much stronger approach. Or as Ms. McCarthy put it, “We did not want to create a crisis center if it operated in a silo. We wanted it to be embedded in the existing continuum, and we wanted to make sure that transitions and referrals happen seamlessly and together.”