
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
One of the most common models for integrating primary and behavioral health services is the Psychiatric Collaborative Care Model (CoCM). And the use of the model is growing. Between 2018 and 2024, the number of commercially insured consumers involved in the model increased 40-fold nationally, from 3,814 to 153,356 (for children and adolescents, the increase was 148-fold). This equates to 317 per 100,000 consumers with a behavioral health diagnosis—up from 12 per 100,000 in 2018. This was one of the findings of a new analysis—Progress Report: Psychiatric Collaborative Care Model.
But utilization of the CoCM model varies widely by state. For example, in Arizona the use of the model was 1,304 per 100,000 commercially insured consumers with a behavioral health diagnosis. But in 16 states, utilization of the model was less than 50 per 100,000.
The average CoCM episode lasts approximately 4.1 months with an average reimbursement of $475 to $650 for Medicare and Medicaid, assuming reimbursement at 100% of Medicare levels. In commercial health plans, the reimbursement was approximately $760 to $1,040 for commercial plans, assuming reimbursement at 160% of Medicare levels. But reimbursement rates vary by state. The average commercial CoCM reimbursement as a percentage of Medicare reimbursement ranged from as high as 277% in California to as low as 90% in Hawaii.
The authors of the analysis attribute the state variance in utilization to a few factors. In many states, Medicaid fee-for-service and many Medicaid health plans do not provide reimbursement for the model. And this restrictive Medicaid reimbursement drives low use among consumers with all types of insurance. Other state factors driving differences in utilization include variance in consumer “out-of-pocket” expenses and the requirement for provider organizations to use code G0512 for billing.
Despite the geographic variance, the growth of the CoCM illustrates the interest of payers and health plans in increasing the use of integrated services. For provider organization executives, the key is find the right “blueprint” for a whole person care strategy that can grow in scale and succeed financially.
We recently heard how one organization did just that in the OPEN MINDS Executive Roundtable, Operationalizing Whole Person Care: The VOAMASS Practical Blueprint For Integrated Service Delivery. Charles E. Gagnon, President and Chief Executive Officer, and Mindy Miller, Chief Operating Officer of Volunteers of America of Massachusetts (VOAMASS) discussed how they took integrated care from concept to operational success.
VOAMASS is a $39.2 million affiliate of Volunteers of America, a national human services organization with 30 affiliates. VOAMASS provides mental health, addiction, homelessness, unemployment, justice-involved, and veteran services, employs approximately 200 staff, and serves approximately 3,400 consumers annually.
The VOAMASS team faced a problem—it was doing good work inside of separate programs, but consumers with multiple needs were a challenge to serve. Their consumers receiving therapy struggled with employment and housing; consumers with housing struggled to connect with social services; and consumers who gained employment were often under paid and struggled with housing.
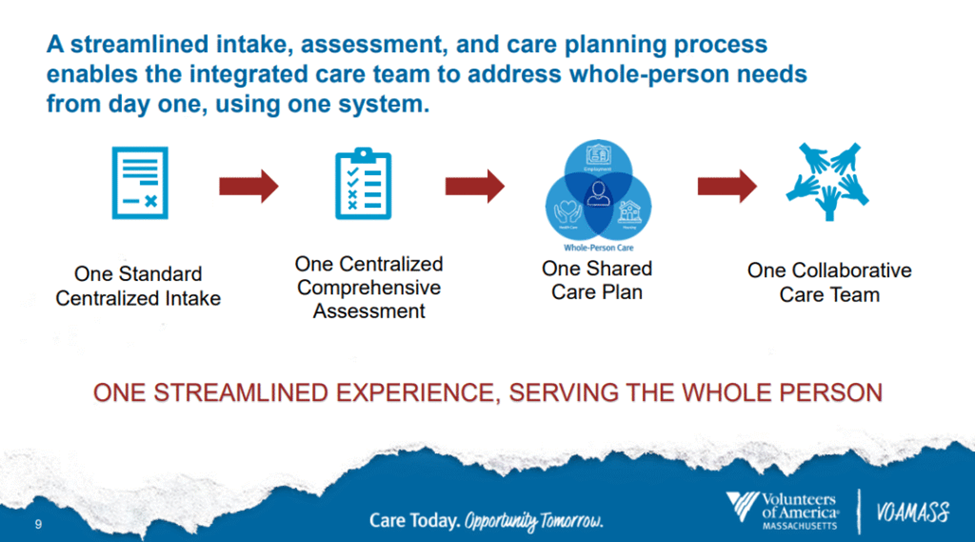
Mr. Gagnon and Ms. Miller saw integrated care as the solution. They designed a model where every consumer would have access to health care, housing, and employment services—delivered by a coordinated, cross-disciplinary care team. To do this, the organization applied for Substance Abuse and Mental Health Services Administration (SAMHSA) grants and used the funding to centralize intake, assessment, and care planning. To support this new intake and service approach, they redesigned the documentation and data infrastructure for better efficiency and data capture.
The VOAMASS executives discuss the multiple effects that this new model has had on the organization and the consumers they serve. From the consumer perspective, there is now a more streamlined consumer experience, with a streamlined intake process and better identification of consumer needs. And with better needs identification, the number of services provided increased by 50% after the launch of the model.
Analyzing the integrated data from the new model, the management team identified the need for more services for co-occurring conditions and converted all four of its residential programs to higher-acuity co-occurring programs. With that change to more intensive programming, the reimbursement move from $179 to $291 per person per day to $363 per person per day across all four programs.
The VOAMASS executives offered two key pieces of advice for executives considering adopting new integrated care models. One is the need for the management team to be open to breaking down service line silos. The other is to deliberately design an operationally and financially sustainable model in order to take the program to scale.
They noted that for whole person care models to succeed, leaders must support a plan that breaks down service line silos. This is done by redesigning workflows around the consumer served, not around program boundaries. This “one-stop-shop” approach also means adopting one shared care plan for the consumer and one cross-disciplinary team that can support that consumer regardless of what services are needed.
“We were doing really great, but if we could get all of these different things in the organization to work together, break down the silos, we can do even better,” said Ms. Miller. “One shared team comes together, with people from each part of our lines of business, and we wrap around the person to make sure that it’s one collaborative team and that everybody knows what the plan is.”
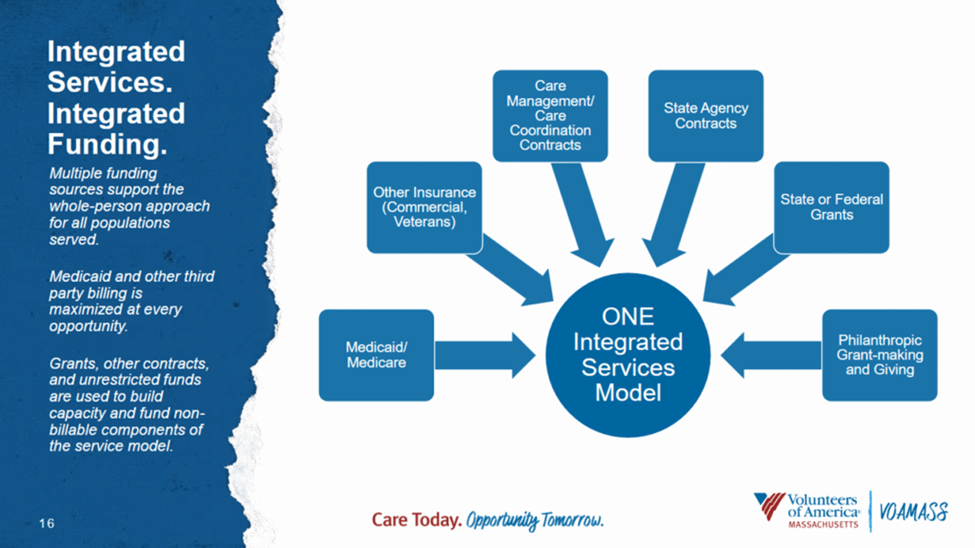
Secondly, whole person care models must be both operationally and financially sustainable in order to scale. This includes getting the staff on board with the operating model—a shared care plan and shared care coordination. But it also means creating financial models to understand opportunities for service reimbursement, likely combining different funding sources to pay for parts of the model that aren’t billable.
“We could not have done this unless we had total buy-in,” said Mr. Gagnon. “And we really needed to think of approaches for getting funding that supports whole person care. Multiple funding sources are needed to support the model for all of the populations we serve, not just some.”
The prospect of growth through creating more whole person care models—with more value-based reimbursement—may seem daunting. As Ms. Miller put it, “You need to be able to dream and fail a little bit and then have flexibility to be able to pivot. It was a lot taking chances and knowing that we weren’t going to do it perfectly the first time. That is absolutely in the core of what you would need in your executive team—willing to be flexible and also change.”