
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
NCQA recently announced they will be expanding their work with federally qualified health centers (FQHCs) and FQHC look-alikes this year. There are already 3,200 health centers that have earned the Patient-Centered Medical Home (PCMH) Recognition from NCQA. But going forward, NCQA will be expanding their work with health centers to include the NCQA Distinction in Behavioral Health Integration—NCQA Is Recruiting Federal Health Centers To Participate In HRSA-Funded Program. The program expansion is being funded by the Health Resources & Services Administration through a new task order.
The Distinction in Behavioral Health Integration recognition will be awarded to PCMH programs with enhanced competencies in serving behavioral health. The recognition is based on 18 criteria across four domains: integrating a behavioral health workforce, enabling information sharing, implementing evidence-based protocols, and using quality measures to track outcomes. According to the NCQA, this is a framework for translating whole person care from concept into daily operations.
The strategic implication of this evolution is significant for specialty provider organizations. By building the capacity to meet these requirements, primary care organization are positioning themselves to manage more of the service continuum for consumers with behavioral disorders and cognitive disabilities.

This is critical because health plan executives are shifting toward more ‘whole person’ approaches to managing care. For example, Centene has introduced a behaviorally-led primary care model in the Florida market.
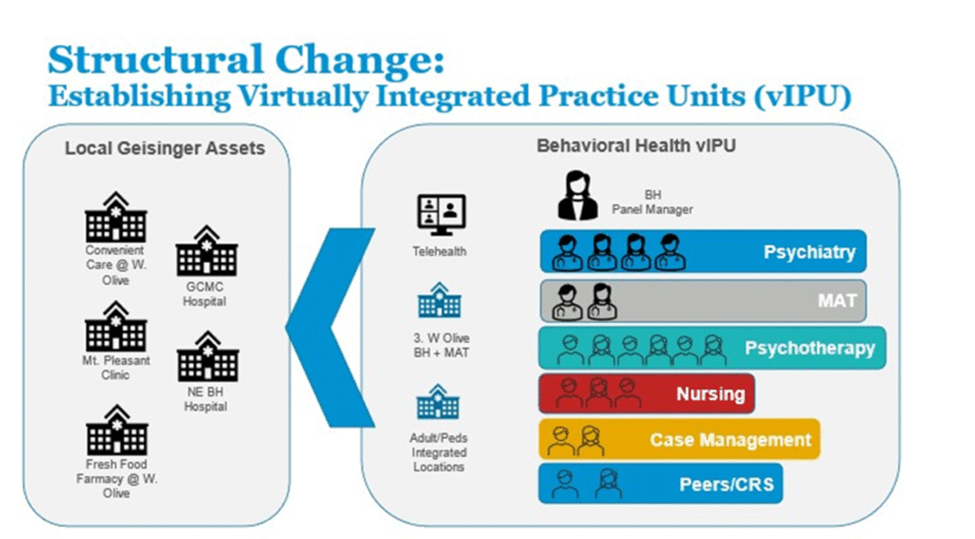
Another example of health plan development is at Geisinger, where Integrated Practice Units have been developed for operationalizing whole person care and, Optum has introduced their integrated behavioral health home model.
And there have been and continue to be many models focused on integrated care at the federal level.
In addition, there have been many models focused on integrated care at the federal level. Most recently, the Trump Administration has introduced the Make America Healthy Again: Enhancing Lifestyle and Evaluating Value-Based Approaches Through Evidence Model—known as ELEVATE—a voluntary initiative designed to test lifestyle and functional medicine interventions that are not currently covered by Medicare fee-for-service.
I asked my colleague, Margaret Mays, senior associate at OPEN MINDS, about the implications of this development. “This demonstrates to health plans, community organizations, and other stakeholders that your PCMH meets the gold standard when it comes to standardized tools and evidence-based practices in behavioral health,” she said. “It shows that you’ve developed a care model that’s fully integrated, dedicated to whole person care.”
“PCMH’s focus and foundation is on team-based, data-driven care, population health, and care coordination. That is all in line with value-based agreement components of risk-sharing and pay-for-performance quality metrics. It has a direct tie to VBC and contracting. The patient-centered medical home has been shown to increase outcomes and lower costs using valid and reliable measures.”
For specialty provider organizations, the challenge is to build primary care service delivery capacity. “Behavioral health organizations need to first identify primary care partners in their market and begin building collaborative models—whether that’s through warm handoffs, co-location, or shared care teams. At the same time, they need to assess their readiness for delivering primary care and integrated services, including how data is shared, how teams communicate, and how roles are defined across providers. This includes understanding the behavioral health integration billing codes and how those impact reimbursement. Without that, even well-designed models can be difficult to sustain.”
Provider organizations that embrace the integration of physical and behavioral health will be better positioned for sustainability and growth. Those that do not may find it increasingly difficult to compete in a market that is rapidly shifting toward integrated, performance-driven models of care. As Ms. Mays emphasized, “Executives need to embrace the concept integrated service delivery, be flexible in the model design, and create models for consistent and accessible communication. That’s what allows teams to work together effectively to deliver whole person care.”