
By Monica E. Oss, Chief Executive Officer, OPEN MINDS
Telehealth isn’t going away. But it isn’t taking over, either.
The question for health plan and provider organization executives is no longer whether to offer virtual care. The question is what delivery model will define the next decade—and how much infrastructure to build around each modality.
A recent study of behavioral health treatment patterns among U.S. service members offers some clarity. Among individuals receiving care for 12 behavioral health conditions, 60% received in-person care only, 4% received telehealth only, and 36% received hybrid care.
Hybrid (not virtual-only) is the growth story.
And the utilization patterns are telling. Consumers receiving hybrid care had three times as many visits as those receiving in-person care only—and eight times as many as those using telehealth only. Visit intervals were also slightly shorter in hybrid and telehealth modalities.
This isn’t a telehealth-versus-office debate. It’s a signal that consumers use care differently when access expands. Hybrid care appears to drive higher engagement and more frequent touchpoints—particularly for conditions like ADHD, PTSD, major depressive disorder, and generalized anxiety disorder.
For executive teams planning workforce models, real estate strategy, and technology investments, this matters. Hybrid capacity planning is not about duplicating services across two settings. It’s about designing systems that allow care to flex based on acuity, engagement, and access.
But hybrid only solves part of the access equation.
We explored the boundaries of hybrid care at The 2025 OPEN MINDS Service Excellence Institute during the session Innovations In Virtual & Non-Traditional Service Delivery With Brightside Health & The LA Department Of Mental Health. Two organizations. Two very different models. One shared lesson: care delivery is no longer location-based—it is population-based.
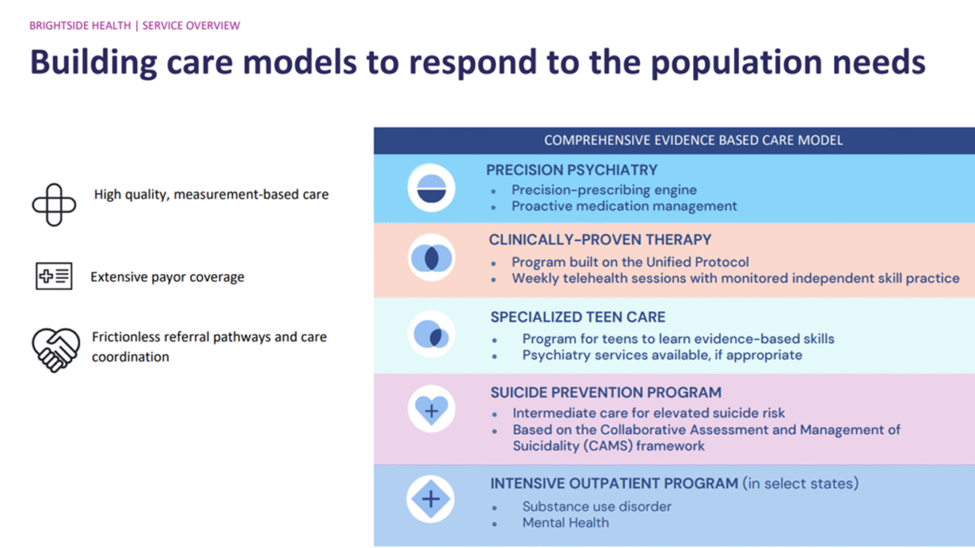
provider within 48 hours. The organization offers medication management, evidence-based therapy, virtual intensive outpatient services, teen programming, and a structured Suicide Prevention Program. Commercial insurance, Medicare, Medicaid, and subscription-based self-pay options are accepted, broadening access beyond traditional in-network models.
“Our EHR is our clinic,” explained Erin O’Callaghan, Ph.D., senior director of therapy programs & quality, and Melissa Matos, Ph.D., director of therapy programs.
The Suicide Prevention Program is particularly notable. It serves adults with active suicidal ideation, including those recently discharged from emergency departments, a population often lost to follow-up. Same-day and next-day appointments are available, and treatment relies on cognitive behavioral therapy, structured social support, and stigma reduction.
And the outcomes are notable. Of nearly 26,000 people treated in California, 34% presented with active suicidal ideation. Among those individuals, 72% experienced a reduction in ideation within 12 weeks and 47% reported no suicidal ideation after 12 weeks. One-third improved by the fourth session. Participants remain in one coordinated ecosystem, reducing fragmentation between crisis response and ongoing care.
The strategic insight is not simply that virtual care works. It’s that certain populations can be served effectively, quickly, and at scale through a precision virtual model.
But that model does not reach everyone.
For individuals with serious mental illness (SMI) experiencing homelessness, virtual care is not an option. That is where the Los Angeles County Department of Mental Health’s Homeless Outreach Mobile Engagement (HOME) program enters the picture.
During the session, Dan Mansfield, mental health program manager II, Aubree Lovelace, division chief, and Shayan Rab, M.D., associate medical director, explained how the HOME model was designed to meet people who will never log into a patient portal.
The HOME team provides in-community street psychiatry—meeting individuals where they are, building trust, delivering food, water, clothing, and clinical care. Psychiatric assessments happen in the field. Medication decisions are made there. Housing is the stabilization goal when possible.
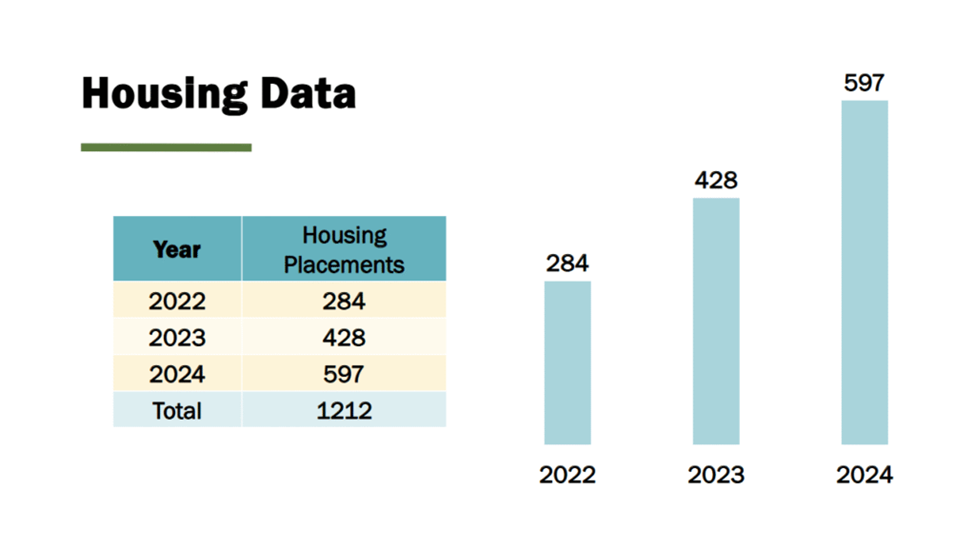
In 2024, the HOME program served 2,519 individuals and placed 597 in housing. Police drop-offs have decreased, transfer-of-custody time has shortened dramatically, and most individuals hospitalized are discharged to housing or residential treatment rather than returning to the street.
This is not hybrid care. This is beyond the office entirely.
And the leadership lesson is not just clinical, it is operational persistence. As Ms. Lovelace noted, building trust can require repeated contact and long time horizons. “Get creative—and remember our clients need us now more than ever.”
Taken together, these two models illustrate a larger strategic shift. Behavioral health delivery is fragmenting, not consolidating, across modalities.
Some consumers require fully virtual precision psychiatry. Many benefit from hybrid flexibility. The most vulnerable require in-community, nontraditional care.
Designing around a single modality creates strategic risk.
Workforce planning must reflect multiple delivery environments. Capital allocation must balance technology investment with community partnerships. Leadership teams must deliberately architect how these modalities connect operationally and financially.
The future of behavioral health is not virtual or in-person. It is responsive.